Volume 2, Issue 3
To What Extent Can Herbal Interventions Reduce Benzodiazepine Reliance and Overmedication in Alcohol Withdrawal Syndrome (AWS)
By Sydney McCoy

is a fourth-year Psychology student. Their research area focuses on the extent to which herbal interventions can improve patient outcomes, with a focus on those with psychiatric and neurological comorbidities. . Her research advisor is Dr. Erika Montanaro from the College of Humanities & Earth and Social Sciences
Abstract
Alcohol use disorder is a common condition that afflicts large populations within the United States. A subset of individuals who report alcohol use disorder develop alcohol withdrawal syndrome after abrupt cessation from alcohol, resulting in severe physiological consequences. Benzodiazepines are first-line treatments for instances of withdrawal; despite general efficacy, benzodiazepines pose large-scale concerns of dependency. The risks of benzodiazepine treatment present a need for an integrative treatment methodology. This literature review attempts to investigate solutions to benzodiazepine reliance, utilizing herbal interventions through neuropsychological and clinical psychology perspectives. Neuropsychology identifies withdrawal mechanisms, whilst clinical psychology addresses behavioral antecedents that vary in treatment. Integrative approaches aid in the evaluation of alternative treatments like Ashwagandha and Purple Passion Flower, revealing the adjunctive role of herbal interventions in clinical settings. Significant gaps within the literature give way to larger issues regarding benzodiazepine administration guidelines and the lack of integrative herbal interventions. The medical system’s reliance on benzodiazepines may contribute to an increased risk of reliance among patients with alcohol withdrawal syndrome, and without reformation, this issue will persist.
AWS, AUD, Ashwagandha, Passiflora incarnata L. Benzodiazepines, Purple Passion Flower, Withania somnifera
Introduction
Alcohol is one of the most commonly utilized substances within the United States, with over 75 percent of individuals over the age of 12 reporting lifetime consumption (National Institute on Alcohol Abuse and Alcoholism, 2024). Those who report lifetime consumption struggle with Alcohol Use Disorder (AUD), often characterized by the problematic use of alcohol marked by physiological dependence, hazardous use, and failure to fulfil obligations (American Psychiatric Association, 2013). Those who experience negative effects of AUD seek remission through halting alcohol consumption to improve their quality of life (Cooper & Vernon, 2012). Although abrupt discontinuation is associated with certain health benefits, complete cessation can lead to a subsequent condition known as Alcohol Withdrawal Syndrome (AWS). Shortly after the onset of AWS, mild to moderate symptoms like anxiety, tachycardia, and headache arise, with critical symptoms emerging 48 hours after the onset of alcohol cessation (Martin et al., 2018). Severe symptoms of AWS include alcohol hallucinations (visual and auditory) and seizures that require hospitalization for intensive care and supervision. These critical conditions affect large populations, as 50% of individuals with AUD experience AWS (Celik et al., 2024), with an increasing number of hospitalizations emerging per year.
Given the widespread impact of AWS among those diagnosed with AUD, standards of care surrounding alcohol withdrawal follow strict guidelines. Treatment protocols encompass preliminary objectives to ensure individuals suffering from withdrawal have a safe, humane, and recovery-oriented detox. The first step to AWS treatment is identification and severity assessment of the Clinical Institute Withdrawal Assessment of Alcohol Scale Revised (CIWA-Ar) (Sullivan et al., 1989; see Appendix A). This scale provides a reliable way to assess the severity of alcohol withdrawal in patients through the examination of critical patient history, including previous history of severe withdrawal, hospitalizations for alcohol withdrawal, and duration of abstinence (Alvanzo et al., 2020). In this stage, individuals are ranked on a scale from mild to severe/complicated alcohol withdrawal severity. Individuals with varying levels of severity are then provided with corresponding levels of care.
Benzodiazepines are first-line treatments for AWS as they are positive allosteric modulators that enhance a given receptor’s effects via binding to an alternate site on the receptor, distinct from the main agonist site (Hackos & Hanson, 2017). Benzodiazepines bind to the GABAA receptor in the brain to counteract severe symptoms of withdrawal by enhancing the inhibitory nature of the receptor. As a result, symptoms such as seizures and delirium (Martin et al., 2018) are minimized during AWS treatment. The depressive nature of benzodiazepines results in anxiolytic, hypnotic, anticonvulsant, and muscle-relaxing effects (Votaw et al., 2019), optimal for neutralizing severe withdrawal symptoms. Despite the effectiveness of benzodiazepines, concerns still arise with their use, as the psychoactive drug can create an issue of dependence in those who receive them as a crucial form of treatment. Notably, 30 percent of individuals with AUD report benzodiazepine misuse (McHugh et al., 2020). This cycle of adopting differing instances of dependence is often known as cross-addiction or sequential dependence, where one recovers from an addiction to develop a dependence on a secondary substance after initial treatment (Dowd et al., 2022). Thus, these findings have prompted the evaluation of benzodiazepine safety within clinical settings. In a broader context, these findings reflect patterns of Western or conventional medicinal approaches that prioritize pharmaceutical and procedural interventions (Yoshinaga et al., 2020). Although these approaches have been proven to be effective with substantial research, some interventions have been associated with risks of dependency and adverse physiological effects.
Instances of benzodiazepine reliance and misuse are not solely dependent on the patient, but rather the shared responsibility of regulatory healthcare guidelines and administration. A prime example of this interplay can be examined during the application of excessive loading procedures. Loading doses are high doses of a particular drug, often administered to elicit an immediate clinical response (Miniaci & Gupta, 2020), typically used in cases requiring anticonvulsant or severe pain management. This administration technique typically occurs under a front-loading regimen, entailing the administration of a loading dose at the beginning of treatment to compensate for a medication’s long half-life, as longer half-lives delay when therapeutic effects take place. Although these procedures effectively manage delirium treatments, convulsions, and autonomic hyperactivity, it can also lead to an increased risk of reliance depending on the loading dose procedure utilized (Sujatha et al., 2017).
As different alternatives to benzodiazepines are being considered due to AWS, given their potential for adverse effects, the integration of herbal interventions may be a suitable alternative in reducing benzodiazepine dependence by enhancing therapeutic efficiency, hence reducing the amount of benzodiazepines needed during treatment and subsequently reducing benzodiazepine reliance. Herbal medications are often used adjunctively with other medications worldwide, although Western civilizations present with apprehension in adopting integrative approaches (Mohammad Hadi Nematollahi et al., 2022). Skepticism continues to follow herbal medication in westernized medicine; however, limited research has been conducted (Chen & Lader, 1990) and presented on the topic to justify the hesitation to use alternatives to benzodiazepines to treat AWS.
Perspective #1: Neuropsychology
The physiological basis of withdrawal is primarily due to the disruption of homeostasis in the central nervous system (CNS) following subsequent detoxification. The CNS is the body’s processing and control system, consisting of the brain and the spinal cord (Cleveland Clinic, 2023). This system acquires sensory information from the nerves and responds to this input via the transmission of electrical signals through the spinal cord. γ-Aminobutyric acid (GABA) and glutamate are important neurotransmitters that play opposing homeostatic roles in the CNS. GABA is a primary inhibitory neurotransmitter in the CNS that reduces neural hyperexcitability (Cleveland Clinic, 2022a), whilst glutamate is the most excitatory neurotransmitter in the brain that promotes transmission by increasing the likelihood of action potential initiation (Cleveland Clinic, 2022b). Chronic alcohol indulgence tends to provoke a “tipping of the scales,” as GABA production and potency increase, while simultaneously suppressing glutamate. This indulgence leads to a state of inhibitory dominance or disinhibition characterized by a reduction of cognitive control and “inability to suppress impulsive behaviors” (Field et al., 2010). Chronic alcohol cessation can shift the body’s neurochemical composition from disinhibition to a state of hyperexcitability. This phenomenon is due to the body’s homeostatic rebound effect, causing glutamate overproduction to take place, compensating for long-term suppression of excitatory systems (Brousse et al., 2012). Hyperecitability of the CNS can cause anxiety, agitation, and seizures, commonly seen in cases of AWS (Gilpin & Koob, 2024).
In serious cases of AWS, CNS hyperexcitability can lead to a life-threatening condition known as delirium tremens. Delirium tremens is a fatal form of AWS that is characterized by a set of symptoms including tremors, delirium, diaphoresis, seizures, hyperthermia, and tachycardia (Cleveland Clinic, 2023a). Preexisting mental health conditions increase the risk of delirium tremens development by enhancing one’s CNS excitability. Enhanced stress responses from preexisting conditions, coupled with neurochemical imbalances caused by alcohol withdrawal, can induce harmful levels of CNS hyperactivity. This level of hyperexcitability can result in a higher risk of delirium tremens development (Bramness et al., 2022). Delirium tremens can contribute to several complications during AWS treatment, including cardiovascular system distress, neurological dysfunction, and seizures (Mulkey & Olson, 2020). These complications increase mortality risks during AWS treatment, prompting the use of benzodiazepines to quickly decrease withdrawal severity and patient mortality rates.
In cases of AWS, benzodiazepines quickly diffuse through the blood-brain barrier to increase GABA production, decreasing the overexcitation of the CNS while maintaining a temporary balance between inhibitory and excitatory bodily systems. Acute use of benzodiazepines maintains a temporary balance between inhibitory and excitatory systems, although prolonged use can yield considerable health issues. According to Ritvo et al. (2023) in their meta-analysis of long-term benzodiazepine-induced neurological dysfunction, individuals who employed long-term benzodiazepine use experienced symptoms such as memory loss, nervousness, and anxiety even after a year-long discontinuation from the drug. Other physiological and psychological impacts of prolonged benzodiazepine use would include Benzodiazepine-Induced Neurological Dysfunction (BIND), causing an increase in suicidality, akathisia or intense restlessness (American Association of Psychiatric Pharmacists, 2025), and other cognitive deficits similar to those seen in those with AUD.
The physiological consequences of benzodiazepines underscore the importance of an investigative search for a medication with lower risks of dependency with similar GABAergic effects. Herbal medications may be an avenue to pursue, as herbal substances have the potential to reduce dependence due to their synergistic nature (Ali et al., 2022). Being that AWS prompts GABA and glutamate dysregulations, herbs capable of temporarily reinstating homeostasis through manipulating the impacted pathways are an enticing alternative. Passiflora incarnata L., or “Purple Passionflower,” is a promising option, as it benefits those who need GABAergic treatments with no rebound, withdrawal, or dependence effects (Carminati et al., 2024). However, this treatment may not be strong enough to prevent critical neurological events like seizures and may limit its efficacy to instances of tapering. Similarly, Ashwagandha may be another alternate contender for benzodiazepine replacement or adjunct. In the study, Ruby et al. (2012), two groups of mice undergoing alcohol cessation were either given a (1 mg/kg) dose of diazepam (a subclass of benzodiazepine) or (500mg/kg) of Ashwagandha. The study found that (500mg/kg) of Ashwagandha demonstrates potential as a reliable alternative to benzodiazepines under conditions of withdrawal. Moreover, the key to finding an effective herbal alternative, adjunct, or tapering mechanism to benzodiazepines relies on an extract’s interaction with GABA or glutamate within the human brain. While many herbal medications have great sedative properties, they are not strong enough to decrease severe medical events as seen in AWS, limiting their efficacy to adjunctive means. Passiflora incarnata L. consists of GABAergic flavonoids such as chrysin, vitexin, and apigenin, which act as less potent positive allosteric modulators in comparison to benzodiazepines (Elsas et al., 2010). Although the herb exhibits similar inhibitory effects, its slower onset and lower potency may limit its use during severe and urgent cases of AWS. Similarly, Ashwagandha presents with similar barriers, as its GABAergic withanolides act as weak modulators to the GABAA receptor (Haque et al., 2021). Rather than acting as a direct agonist through strong positive allosteric mechanisms, Ashwagandha primarily acts as an adaptogen with mild sedative properties. The literature presented on the topic of benzodiazepines and herbal medicines is quite limited, as the broader scope of herbal medicine integration remains a niche topic with large deficits. Further research regarding herbal medicine integration as a whole requires further expansion, especially within the realm of psychology and the physiological manifestations of mental diseases.
Perspective #2: Clinical Psychology
AUD is often associated with many behavioral antecedents that affect AWS treatment. Specifically, the severity of AWS is often contingent upon concurrent addictive substance use, positive blood alcohol concentration during withdrawal, and co-occurring psychiatric disorders (Alvanzo et al., 2020). Being that alcohol acts as a common depressant of the CNS, varying behavioral factors can affect the effectiveness of particular treatment options within clinical settings (Alvanzo et al., 2020). Consequently, those who present with AUD and other mental health concerns during alcohol cessation are likely to experience psychiatric complications of delirium tremens (Alvanzo et al., 2020). These complications are often reduced by the use of benzodiazepines during severe withdrawal episodes, although it is important to weigh the positive and negative effects of benzodiazepine intervention, as there is a risk of developing secondary dependence. Those with complex cases of AWS require rapid CNS suppression, which herbal interventions may not be able to provide as a result of weaker GABAergic effects and slower medicinal onset. Although the use of herbal interventions may be inappropriate during acute AWS treatment, especially for those with complex cases, their use presents as being the most optimal once care shifts its focus to stabilization and dependence reduction (Haque et al., 2021). Passiflora incarnata L. and Ashwagandha both act as GABA modulators with anxiolytic effects. Utilization of these interventions during benzodiazepine tapering not only acts as a mild anticonvulsant but also as an anti-anxiety agent that cross-tolerates with alcohol to reduce residual CNS excitability (Wolf et al., 2020). The reduction of CNS excitability may also reduce psychological symptoms that present with AWS, including agitation, irritability, and dysphoric mood. The use of adjunctive herbal interventions during the tapering process can aid the management of psychological symptoms, promoting treatment adherence and optimal patient outcomes (Sarkhel et al., 2020).
Systematic guidelines and treatment plans for clinical providers are one of the primary methods to prevent benzodiazepine overuse in those with AUDs (Alvanzo et al., 2020), and current guidelines do not comprehensively address the negative consequences associated with benzodiazepine overuse. Severe CNS depression, following impaired cognition, hypotension, bradycardia, and paradoxical reactions like agitation and combativeness, are common symptoms of benzodiazepine overuse. These symptoms are often harder to treat, given that those who acquire secondary or “transfer addiction” are more likely to experience issues with treatment adherence, reduced quality of life, and pessimistic outcomes (Dennis & Scott, 2007).
Although benzodiazepines can be largely effective when utilized precisely, consistent monitoring and systematic guidelines must be followed to ensure those receiving treatment do not become dependent. Similarly, the distinction of benzodiazepine subclasses and appropriate dosing regimes is essential for this very reason. For example, long-acting benzodiazepines are often recommended over those that are shorter-acting due to their tapering ability that slowly weans the patient off of the medication (Alvanzo et al., 2020). Without the distinction between the two subclasses, individuals may be prescribed short-acting benzodiazepines such as lorazepam or oxazepam, which may wear off quickly, increasing the chances of subsequent addiction (Edinoff et al., 2021). Careful revision and application of new clinical guidelines can go a long way in preventing debilitating issues of sequential dependence in those struggling with AWS.
Integration
When both perspectives are examined in tandem, similar deficits regarding the integration of herbal medication in psychology are apparent. Holistic approaches are less frequently utilized and often superseded by pharmaceutical-grade medications (e.g., benzodiazepines) as symptoms become severe or life-threatening (Alvanzo et al., 2020). Furthermore, many clinicians prefer the prescription of medications like benzodiazepines due to stronger evidence of clinical effectiveness (Carminati et al., 2024), decreasing the chances of holistic applications and research.
Neuropsychological approaches have yet to discover a safe and effective integration of herbal care in Western medicine. Although adjunctive applications have been considered in cases of severe conditions, they are seldom employed due to a lack of research (Nematollahi et al., 2022). However, studies have shown that the adjunctive use of herbal extracts during treatment for AWS should be further explored, as these remedies can provide a less addictive alternative to benzodiazepines during AWS (Carminati et al., 2024). Comparatively, although clinical psychology and neuropsychological approaches mildly advocate for the use of herbal interventions, the general effectiveness of pharmaceutical-grade medications is prioritized to avoid fatal outcomes (Mohammad Hadi Nematollahi et al., 2022).
Shifts towards integrative medicine require an integrative approach with an emphasis on clinical administration and physiological processes. Specific dosage regimens and suboptimal prescription guidelines may be the reason for benzodiazepine reliance (Alvanzo et al., 2020), presenting a demand for policy reformation within the healthcare system. An integrative approach should be utilized in reconstructing new administrative guidelines and providing alternative care for those experiencing AWS.
Acknowledgements
I would like to thank my disciplinary honors mentor, Erika Montanaro, for her support throughout the development of this project. She not only guided me through the research and writing process but also encouraged me to submit this work despite my own initial self-doubt. I am especially grateful for her belief in my abilities and for inspiring me to take greater academic and professional risks moving forward.
References
Airagnes, G., Ducoutumany, G., Laffy-Beaufils, B., Le Faou, A.-L. ., & Limosin, F. (2019). Alcohol withdrawal syndrome management: Is there anything new? La Revue de Médecine Interne, 40(6), 373–379. https://doi.org/10.1016/j.revmed.2019.02.001
Ali, H., Ali, D., Almutairi, B. O., Kumar, G., Karga, G. A., Masi, C., & Sundramurthy, V. P. (2022). Synergistic Effect of Conventional Medicinal Herbs against Different Pharmacological Activity. BioMed Research International, 2022, 1–7. https://doi.org/10.1155/2022/7337261
Alvanzo, A., Kleinschmidt, K., Kmiec, J., Kolodner, G., Marti, G., Murphy, W., Tirado, C., Waller, C., Nelson, L., Holt, S., Rastegar, D., Saitz, R., Weaver, M., Jarvis, M., Kotz, M., Novack, D., Pating, D., Pirard, S., Lindsay, D., & Williams, J. (2020). Physician Health Programs National Association of Addiction Treatment Providers National Association of Clinical Nurse Specialists National Commission on Correctional Health Care. https://www.asam.org/docs/default-source/quality-science/the_asam_clinical_practice_guideline_on_alcohol-1.pdf
American Association of Psychiatric Pharmacists (AAPP). (2025). American Association of Psychiatric Pharmacists (AAPP). American Association of Psychiatric Pharmacists (AAPP). https://aapp.org/ed/summit/2024/session/benzo
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. Diagnostic and Statistical Manual of Mental Disorders, 5(5). https://doi.org/10.1176/appi.books.9780890425596
Bramness, J. G., Pandey, S., Moe, J. S., Toft, H., Lien, L., & Bolstad, I. (2022). History of Delirium Tremens in AUD Patients in Treatment: Relationship to AUD Severity and Other Factors. Substance Abuse and Rehabilitation, Volume 13(13), 65–72. https://doi.org/10.2147/sar.s361810
Brousse, G., Arnaud, B., Vorspan, F., Richard, D., Dissard, A., Dubois, M., Pic, D., Geneste, J., Xavier, L., Authier, N., Sapin, V., Llorca, P.-M. ., De Chazeron, I., Minet-Quinard, R., & Schmidt, J. (2012). Alteration of Glutamate/GABA Balance During Acute Alcohol Withdrawal in Emergency Department: A Prospective Analysis. Alcohol and Alcoholism, 47(5), 501–508. https://doi.org/10.1093/alcalc/ags078
Brunner, E., Chen, C.-Y. A., Klein, T., Maust, D., Mazer-Amirshahi, M., Mecca, M., Najera, D., Ogbonna, C., Rajneesh, K. F., Roll, E., Sanders, A. E., Snodgrass, B., VandenBerg, A., Wright, T., Boyle, M., Devoto, A., Framnes-DeBoer, S., Kleykamp, B., Norrington, J., & Lindsay, D. (2025). Joint Clinical Practice Guideline on Benzodiazepine Tapering: Considerations When Risks Outweigh Benefits. Journal of General Internal Medicine. https://doi.org/10.1007/s11606-025-09499-2
Carminati, M., Mattia Tondello, & Zanardi, R. (2024). Passiflora incarnata L., herba, in benzodiazepine tapering: long-term safety and efficacy in a real-world setting. Frontiers in Psychiatry, 15(1471083). https://doi.org/10.3389/fpsyt.2024.1471083
Celik, M., Gold, M. S., & Fuehrlein, B. (2024). A Narrative Review of Current and Emerging Trends in the Treatment of Alcohol Use Disorder. Brain Sciences, 14(3), 294. https://doi.org/10.3390/brainsci14030294
Chen, Y., & Lader, M. (1990). Long-term benzodiazepine treatment: Is it ever justified? Human Psychopharmacology: Clinical and Experimental, 5(4), 301–312. https://doi.org/10.1002/hup.470050403
Cleveland Clinic. (2022a, April 25). Gamma-Aminobutyric Acid (GABA). Cleveland Clinic. https://my.clevelandclinic.org/health/articles/22857-gamma-aminobutyric-acid-gaba
Cleveland Clinic. (2022b, April 25). Glutamate: What it is & function. Cleveland Clinic; Cleveland Clinic. https://my.clevelandclinic.org/health/articles/22839-glutamate
Cleveland Clinic. (2023a, June 5). Temperance movement: Lower alcohol use and avoid delirium tremens. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/25052-delirium-tremens
Cleveland Clinic. (2023b, November 12). Central Nervous System: What Does It Do? Cleveland Clinic. https://my.clevelandclinic.org/health/body/central-nervous-system-cns
Cooper, E., & Vernon, J. (2012). The effectiveness of pharmacological approaches in the treatment of alcohol withdrawal syndrome (AWS): a literature review. Journal of Psychiatric and Mental Health Nursing, 20(7), 601–612. https://doi.org/10.1111/j.1365-2850.2012.01958.x
Dennis, M., & Scott, C. (2007). Managing Addiction as a Chronic Condition. Addiction Science & Clinical Practice, 4(1), 45–55. https://doi.org/10.1151/ascp074145
Dowd, B., Hein, K., Diez, S. L., Prokofieva, M., Kannis-Dymand, L., & Stavropoulos, V. (2022). Cross-Addiction Risk Profile Associations with COVID-19 Anxiety: a Preliminary Exploratory Study. International Journal of Mental Health and Addiction, 22(106–129). https://doi.org/10.1007/s11469-022-00862-6
Edinoff, A. N., Nix, C. A., Hollier, J., Sagrera, C. E., Delacroix, B. M., Abubakar, T., Cornett, E. M., Kaye, A. M., & Kaye, A. D. (2021). Benzodiazepines: Uses, dangers, and clinical considerations. Neurology International, 13(4), 594–607. https://doi.org/10.3390/neurolint13040059
Field, M., Wiers, R. W., Christiansen, P., Fillmore, M. T., & Verster, J. C. (2010). Acute Alcohol Effects on Inhibitory Control and Implicit Cognition: Implications for Loss of Control Over Drinking. Alcoholism: Clinical and Experimental Research, 34(8), no-no. https://doi.org/10.1111/j.1530-0277.2010.01218.x
Gilpin, N. W., & Koob, G. F. (2024). Neurobiology of Alcohol Dependence: Focus on Motivational Mechanisms. Alcohol Research & Health, 31(3), 185. https://pmc.ncbi.nlm.nih.gov/articles/PMC2770186/
Haque, I. M., Mishra, A., Kalra, B. S., & Chawla, S. (2021). Role of Standardized Plant Extracts in Controlling Alcohol Withdrawal Syndrome—An Experimental Study. Brain Sciences, 11(7), 919. https://doi.org/10.3390/brainsci11070919
International Society of Psychiatric Nurses. (2000). Assessment and Identification Management of Alcohol Withdrawal Syndrome (AWS) in the Acute Care Setting. https://www.ispn-psych.org/assets/docs/10-00-aws.pdf
- Sujatha, T. Arundathi, Rubina, S., B. Ramana, & Nagarajan, G. (2017). DRUG DELIVERY METHODS RANKING ADDICTION POTENTIAL. Semantic Scholar. https://www.semanticscholar.org/paper/DRUG-DELIVERY-METHODS-RANKING-ADDICTION-POTENTIAL-Sujatha-Arundathi/d1764879d5f85a448f04186eefcdcbd9d3320d63
Kang, M., & Ghassemzadeh, S. (2020). Benzodiazepine Toxicity. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK482238/
Khanna, D., Sethi, G., Ahn, K., Pandey, M., Kunnumakkara, A., Sung, B., Aggarwal, A., & Aggarwal, B. (2007). Natural products as a gold mine for arthritis treatment. Current Opinion in Pharmacology, 7(3), 344–351. https://doi.org/10.1016/j.coph.2007.03.002
Kisling, L. A., & Stiegmann, R. A. (2024, February 26). Alternative medicine. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK538520/
Little, H., Donoghue, K., & Drummond, C. (2022). Prolonged benzodiazepine levels following withdrawal in alcohol dependence. Journal of Studies on Alcohol and Drugs, 84(1). https://doi.org/10.15288/jsad.21-00432
Mahesh Kumar Harit, Narendra Mundhe, Sanjay Tamoli, Pawar, V., Vedvati Bhapkar, Ganesh Kolhe, Swapnali Mahadik, Kulkarni, A., & Agarwal, A. (2024). Randomized, Double-Blind, Placebo-Controlled, Clinical Study of Passiflora incarnata in Participants With Stress and Sleep Problems. Curēus, 16(3). https://doi.org/10.7759/cureus.56530
Martin, C. S., Vergés, A., Langenbucher, J. W., Littlefield, A., Chung, T., Clark, D. B., & Sher, K. J. (2018). Algorithm Analysis of the DSM-5 Alcohol Withdrawal Symptom. Alcoholism: Clinical and Experimental Research, 42(6), 1073–1083. https://doi.org/10.1111/acer.13633
McHugh, R. K., Votaw, V. R., Taghian, N. R., Griffin, M. L., & Weiss, R. D. (2020). Benzodiazepine misuse in adults with alcohol use disorder: Prevalence, motives and patterns of use. Journal of Substance Abuse Treatment, 117(10), 108061. https://doi.org/10.1016/j.jsat.2020.108061
Miniaci, A., & Gupta, V. (2020). Loading Dose. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557418/
Mohammad Hadi Nematollahi, Mohammad Ali Ahmadianmoghadam, Mehrnaz Mehrabani, Masoud Moghadari, Adel Ghorani-Azam, & Mehrzad Mehrbani. (2022). Herbal therapy in opioid withdrawal syndrome: A systematic review of randomized clinical trials. PubMed, 14(2), 152–163. https://doi.org/10.22122/ahj.2022.195961.1247
Mulkey, M. A., & Olson, D. M. (2020). Delirium Tremens in the Older Adult. Journal of Neuroscience Nursing, 52(6), 316–321. https://doi.org/10.1097/jnn.0000000000000543
National Institute on Alcohol Abuse and Alcoholism. (2024a, February 27). Alcohol Use Disorder: From Risk to Diagnosis to Recovery | National Institute on Alcohol Abuse and Alcoholism (NIAAA). Www.niaaa.nih.gov. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/alcohol-use-disorder-risk-diagnosis-recovery
National Institute on Alcohol Abuse and Alcoholism. (2024b, September). Alcohol use disorder (AUD) in the United States: Age groups and demographic characteristics. Www.niaaa.nih.gov; National Institute on Alcohol Abuse and Alcoholism. https://www.niaaa.nih.gov/alcohols-effects-health/alcohol-topics/alcohol-facts-and-statistics/alcohol-use-disorder-aud-united-states-age-groups-and-demographic-characteristics
Newman, R. K., Stobart, M. A., & Gomez, A. E. (2024). Alcohol Withdrawal Syndrome. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK441882/
Peschel, W. (2016). Quality Control of Traditional Cannabis Tinctures: Pattern, Markers, and Stability. Scientia Pharmaceutica, 84(3), 567–584. https://doi.org/10.3390/scipharm84030567
Ritvo, A., Foster, D. E., Huff, C., Finlayson, R., Silvernail, B., & Martin, P. R. (2023). Long-term consequences of benzodiazepine-induced neurological dysfunction: A survey. PLOS ONE, 18(6), e0285584–e0285584. https://doi.org/10.1371/journal.pone.0285584
Ruby, B., Benson, M., Kumar, E., Sudha, S., & Wilking, J. (2012). Evaluation of Ashwagandha in alcohol withdrawal syndrome. Asian Pacific Journal of Tropical Disease, 2, S856–S860. https://doi.org/10.1016/s2222-1808(12)60279-5
Sachdeva, A., Choudhary, M., & Chandra, M. (2020). Alcohol Withdrawal Syndrome: Benzodiazepines and Beyond. JOURNAL of CLINICAL and DIAGNOSTIC RESEARCH, 9(9). https://doi.org/10.7860/jcdr/2015/13407.6538
Sarkhel, S., Singh, O., & Arora, M. (2020). Clinical Practice Guidelines for Psychoeducation in Psychiatric Disorders General Principles of Psychoeducation. Indian Journal of Psychiatry, 62(8). https://doi.org/10.4103/psychiatry.indianjpsychiatry_780_19
Shoja, M., Mehri, S., Amin, B., Askari, V. R., & Hosseinzadeh, H. (2018). The Prophylactic and Therapeutic Effects of Saffron Extract and Crocin on Ethanol Withdrawal Syndrome in Mice. Journal of Pharmacopuncture, 21(4), 277–283. https://doi.org/10.3831/kpi.2018.21.031
Steel, T. L., Malte, C. A., Bradley, K. A., & Hawkins, E. J. (2022). Benzodiazepine Treatment and Hospital Course of Medical Inpatients With Alcohol Withdrawal Syndrome in the Veterans Health Administration. Mayo Clinic Proceedings: Innovations, Quality & Outcomes, 6(2), 126–136. https://doi.org/10.1016/j.mayocpiqo.2021.11.010
Sullivan, J. T., Sykora, K., Schneiderman, J., Naranjo, C. A., & Sellers, E. M. (1989). Assessment of Alcohol Withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Addiction, 84(11), 1353–1357. https://doi.org/10.1111/j.1360-0443.1989.tb00737.x
Szilvia Czigle, Nagy, M., Přemysl Mladěnka, & Jaroslav Tóth. (2023). Pharmacokinetic and pharmacodynamic herb-drug interactions—part I. Herbal medicines of the central nervous system. PeerJ, 11(15), e16149–e16149. https://doi.org/10.7717/peerj.16149
Tang, S. W., Tang, W. H., & Leonard, B. E. (2017). Herbal medicine for psychiatric disorders: Psychopharmacology and neuroscience-based nomenclature. The World Journal of Biological Psychiatry, 20(8), 586–604. https://doi.org/10.1080/15622975.2017.1346279
Tidwell, W. P., Thomas, T. L., Pouliot, J. D., Canonico, A. E., & Webber, A. J. (2018). Treatment of Alcohol Withdrawal Syndrome: Phenobarbital vs CIWA-Ar Protocol. American Journal of Critical Care, 27(6), 454–460. https://doi.org/10.4037/ajcc2018745
UF Health. (2025). Benzodiazepine Dependence – UF Health. Ufhealth.org. https://ufhealth.org/conditions-and-treatments/benzodiazepine-dependence
Valenzuela, C. F. (1997). Alcohol and neurotransmitter interactions. Alcohol Health and Research World, 21(2), 144. https://pmc.ncbi.nlm.nih.gov/articles/PMC6826822/
Votaw, V. R., Geyer, R., Rieselbach, M. M., & McHugh, R. K. (2019). The epidemiology of benzodiazepine misuse: A systematic review. Drug and Alcohol Dependence, 200(114), 95–114. http://doi.org/10.1016/j.drugalcdep.2019.02.033
Wolf, C., Curry, A., Nacht, J., & Simpson, S. A. (2020). Management of alcohol withdrawal in the emergency department: Current perspectives. Open Access Emergency Medicine, Volume 12(1), 53–65. https://doi.org/10.2147/oaem.s235288
World Health Organization. (2012). Prevention. Www.who.int. https://www.who.int/teams/mental-health-and-substance-use/treatment-care/mental-health-gap-action-programme/evidence-centre/alcohol-use-disorders/management-of-alcohol-withdrawal
Xu, J., Mercury, J., Zhang, Z., & Xu, F. (2008). Psychological, social and behavioural factors that influence drug efficacy: a noteworthy research subject in clinical pharmacology. British Journal of Clinical Pharmacology, 66(6), 901–902. https://doi.org/10.1111/j.1365-2125.2008.03300.x
Yoshinaga, R., Maki, T., Goto, Y., Inoue, H., Yano, H., & Tahara, E. (2020). Discontinuation or reduction in benzodiazepine use by treatment with the traditional herbal medicine Hangekobokuto, case reports. Journal of General and Family Medicine, 21(4), 143–145. https://doi.org/10.1002/jgf2.313
Appendices
Appendix A
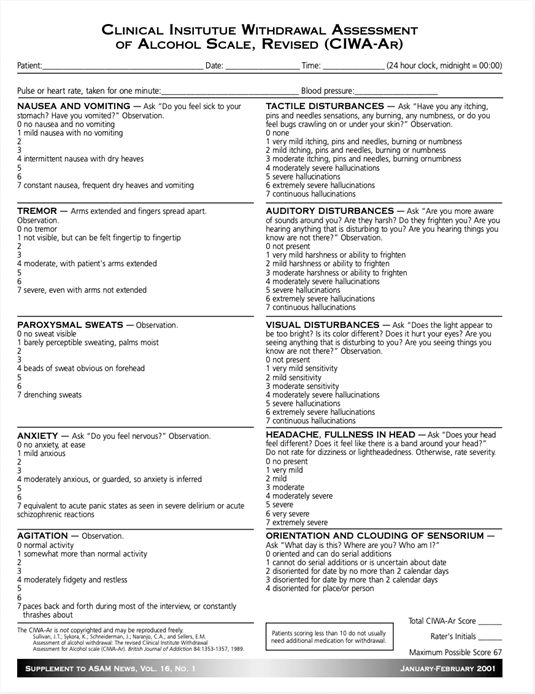
Figure I: Clinical Institute Withdrawal Assessment Of Alcohol Scale, Revised (CIWA-AR)